Shoulder pain is defined as chronic when it has been present for longer than six months.
Common conditions that can result in chronic shoulder pain :
Rotator cuff disorders include tendinopathy, partial tears, and complete tears. A clinical decision rule that is helpful in the diagnosis of rotator cuff tears includes :
Adhesive capsulitis can be associated with diabetes and thyroid disorders.
Clinical presentation includes diffuse shoulder pain with restricted active and passive range of motion on examination.
Acromioclavicular osteoarthritis presents with superior shoulder pain, acromioclavicular joint tenderness, and a painful cross-body adduction test
In patients who areolder than 50 years
GlenohumeralOsteoarthritis usually presents as gradual pain and loss of motion.
In patients younger than 40 years, glenohumeral instability generally presents with a history of dislocation or subluxation events
DIAGNOSTIC CATEGORIES
Acromioclavicular osteoarthritis
Acromioclavicular joint pathology is
Adhesive capsulitis
Adhesive capsulitis refers to a painful shoulder in which the active and passive ranges of motion are severely limited.
Gradual onset of pain and stiffness,
Loss of motion in all planes with increased pain at the extremes of motion, and a
History of diabetes or thyroid disease are consistent with the diagnosis.
Glenohumeral instability
Glenohumeral instability refers to dislocation and subluxation.
The patients are usually younger than 40 years and have a history of dislocation or subluxation events, which is often involved with
Collision or overhead sports.
A “dead arm,” numbness over the lateral deltoid, and a positive apprehension test are consistent with the diagnosis.
Glenohumeral osteoarthritis
Glenohumeral osteoarthritis usually presents as gradual pain and loss of motion in patients older than 50 years.
A history of arthritis,
Previous shoulder surgery, pain, crepitus, and decreased motion is consistent with the diagnosis.
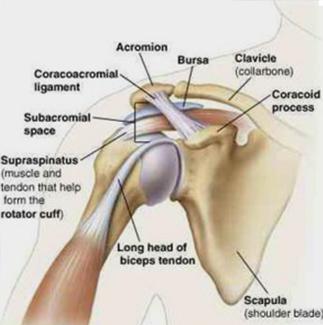
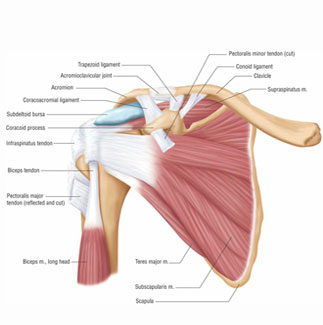
Rotator cuff pathology
Rotator cuff disorders that affect the function of the rotator cuff include a
Partial or complete tear,
Tendinitis or tendinosis, and
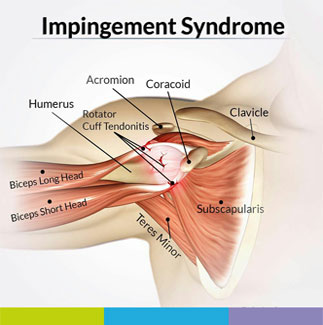
Calcific tendinitis. Initially, it is more important to differentiate this group of disorders from the other groups than it is to identify the specific diagnosis. Typically, the patients are older than 40 years and complain of pain in the lateral aspect of the arm with radiation no farther than the elbow. Weakness, a painful arc of motion, night pain, and a positive impingement sign are components of the history.
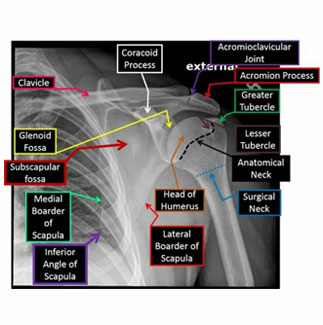
Radiographs can be helpful to diagnose calcific tendinitis, acromial spur, humeral head cysts, or superior migration of the humeral head, but are typically normal.
Other conditions
Numerous other problems that can affect the shoulder are somewhat less common, such as biceps and labral pathology (e.g., SLAP tear—superior labrum anterior to posterior tear—an avulsion injury to the root of the long head of the biceps tendon) and multidirectional instability. Other conditions are extremely uncommon, such as a suprascapular nerve injury, Parsonage Turner syndrome (brachial plexus neuritis), and a neuropathic shoulder from syringomyelia. The shoulder can also be the area of perceived pain for many non-shoulder problems, including fibromyalgia, cervical radiculopathy, and thoracic outlet syndrome. Fibromyalgia is notable for classic areas of tender points. Cervical radiculopathy pain is generally posterior, with radiation to the neck and down the arm below the elbow. Thoracic outlet syndrome, like cervical radiculopathy, is notable for symptoms that extend past the elbow and often into the hand. There can be neurologic or vascular symptoms based on the subtype. Positive radiographs are helpful for diagnosing severe cervical osteoarthritis, but are typically negative. Positive provocative shoulder testing (e.g., Hawkins’ impingement test, empty-can test, external rotation test) that disappears after a subacromial lidocaine injection is inconsistent with the diagnosis of fibromyalgia, cervical radiculopathy, or thoracic outlet syndrome.
MANAGEMENT OF CHRONIC SHOULDER PAIN
Most patients with a chronic shoulder disorder can initially be treated conservatively with some combination of activity modification, physical therapy, medications, and corticosteroid injections, if necessary.
INTERVENTIONAL TREATMENTS FOR CHRONIC SHOULDER PAIN
1.Corticosteroid injections
If patients have a poor response to initial treatment for chronic shoulder disorders, corticosteroid injections combined with a local anesthetic can be administered. The injection needs to be directed toward the affected area, such as the
Patients with adhesive capsulitis have been shown to respond to intra-articular injections with decreased pain and increased function, particularly in combination with physical therapy for stretching.
Intra-articular hyaluronic acid injections have shown promise in several studies on glenohumeral osteoarthritis.
Injection into the acromioclavicular joint can provide some diagnostic information because even short-term relief of symptoms can help confirm the diagnosis.
2.Suprascapular nerve block
The suprascapular nerve block has been utilized for a number of years to address various causes of shoulder pain. Early advocates of the Suprascapular nerve block reported its usefulness in treating
The procedure is done on an outpatient basis. The procedure is performed under ultrasound guidance to ensure accuracy of needle placement. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that there may need repeated injections.
Patients who get temporary relief from suprascapular nerve block may be suitable for suprascapular nerve ablation (pulsed radiofrequency treatment). This is likely to provide longer-term pain relief.
3.Suprascapular Nerve Block
Shoulder pain is common in the community, affecting 15–30% of adults at any one time. Causes include
Evidence for the efficacy of various treatments of shoulder pain is limited. There is little evidence to support or refute the efficacy of common interventions for shoulder pain. From a clinician’s perspective, therapeutic options for the management of chronic shoulder pain are limited. Simple analgesia, non-steroidal anti-inflammatory drugs (NSAIDs), intraarticular steroid injection, and surgery all have their limitations, particularly in older populations with comorbidities.
INDICATIONS FOR SUPRASCAPULAR NERVE BLOCK
Suprascapular nerve block can be used for acute and chronic pain of the shoulder joint from any cause:
TECHNIQUE
The procedure is done on an outpatient basis. The procedure is performed under ultrasound guidance to ensure accuracy of needle placement. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that there may need repeated injections.
Generally a mixture of local anaesthetic and steroid is injected. The local anaesthetic is probably responsible for immediate pain relief, whereas steroids are believed to be responsible for pain relief 2–6 days after their administration. For a diagnostic block, a short-acting anaesthetic alone is sufficient.
4.SUPRASCAPULAR NERVE ABLATION
Patients who get temporary relief from suprascapular nerve block may be suitable for suprascapular nerve ablation (pulsed radiofrequency treatment). This is likely to provide longer term pain relief.
Suprascapular Nerve Ablation
The procedure is done on an outpatient basis. The procedure is performed under ultrasound guidance to ensure the accuracy of needle placement. Specialized equipment including radiofrequency machine, probe, and RF needle is utilized to heat the nerve up to a temperature of 42°C. Generally local anaesthetic is injected around the nerve following nerve ablation. The local anaesthetic is responsible for immediate pain relief, whereas pulsed radiofrequency takes 4 to 6 weeks to provided sustained pain relief. Pain relief from pulsed radiofrequency ablation of the suprascapular nerve can last between 6 months to 24 months.